

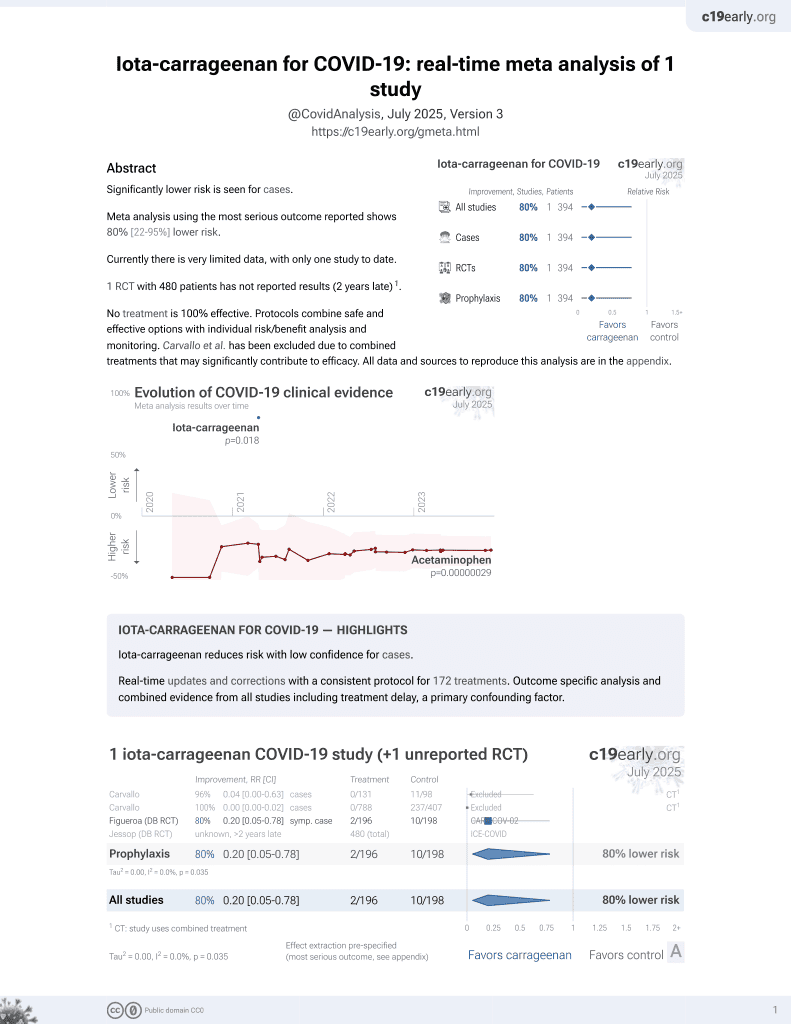
Iota-carrageenan for COVID-19: real-time meta analysis of 1 study
Abstract
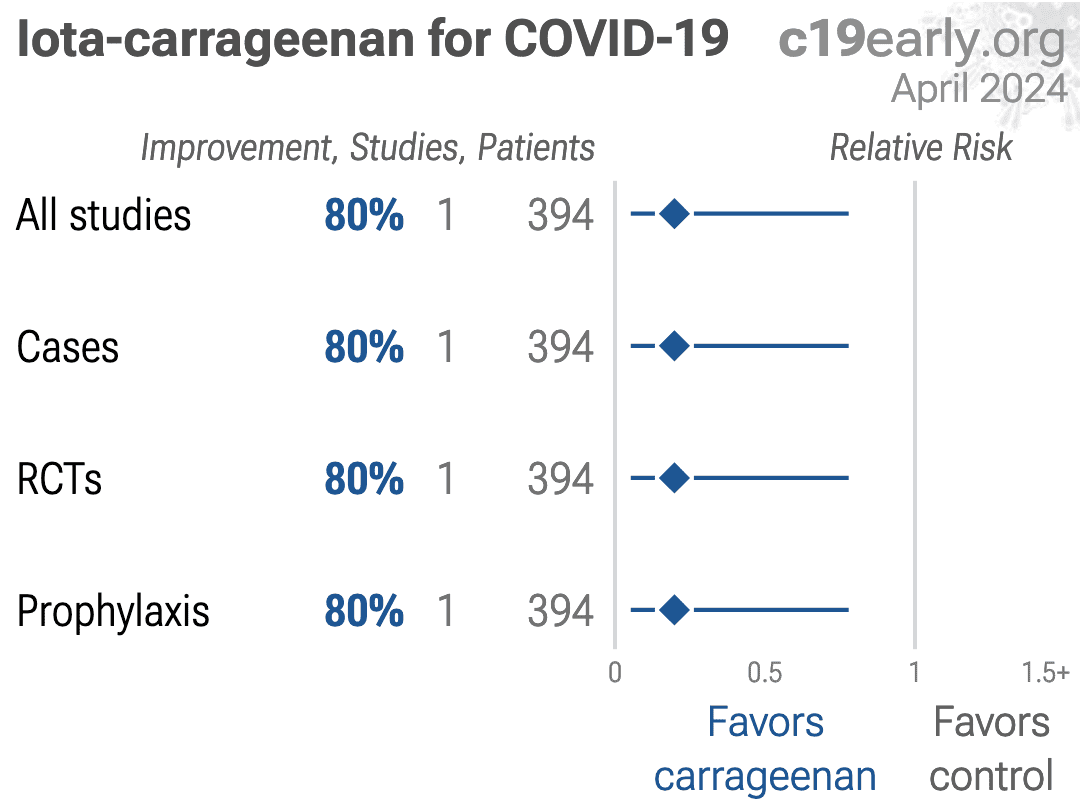
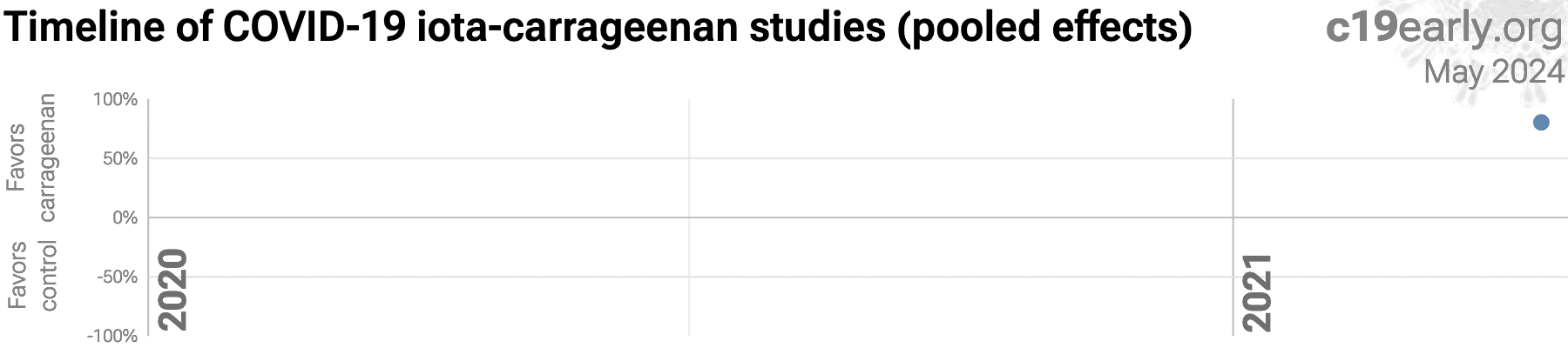
Significantly lower risk is seen for cases.
Meta analysis using the most serious outcome reported shows
80% [22‑95%] lower risk.
Currently there is very limited data, with only one study to date.
No treatment is 100%
effective. Protocols combine safe and effective options with individual
risk/benefit analysis and monitoring.
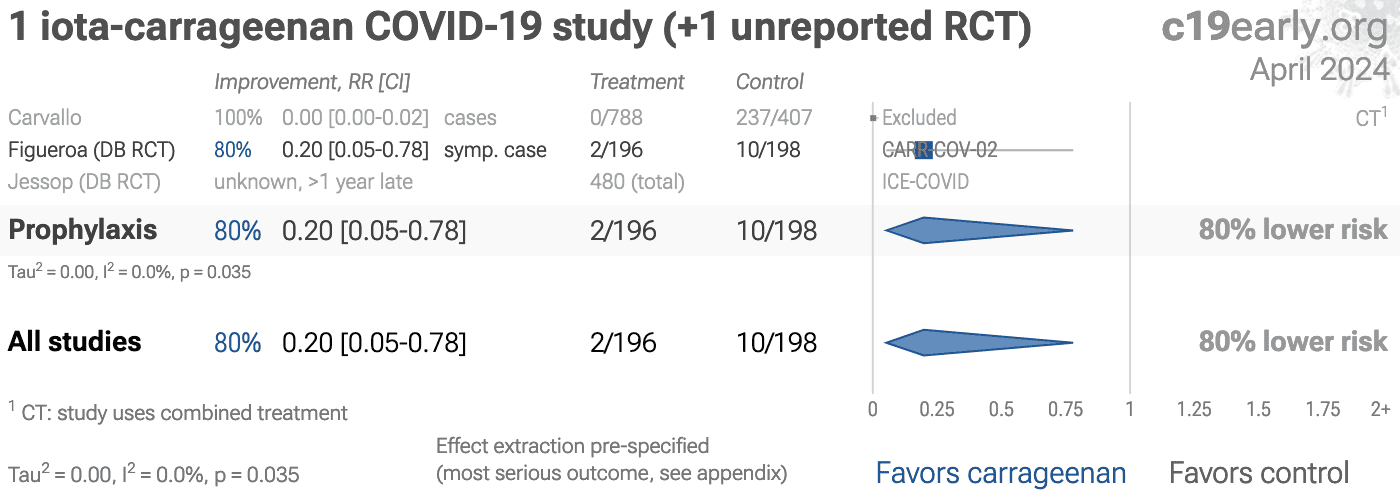
Carvallo et al. has been excluded due to combined treatments that may significantly contribute to efficacy.
All data and sources to reproduce this analysis are in the appendix.
Iota-carrageenan for COVID-19 — Highlights
Iota-carrageenan reduces risk with low confidence for cases.
Real-time updates and corrections with a consistent protocol for 172 treatments. Outcome specific analysis and combined evidence from all studies including treatment delay, a primary confounding factor.
Naso/oropharyngeal treatments
AlkalinizationCetylpyridin..
Chlorhexidine
Chlorphenira..
Hydrogen Per..
Iota-carragee..
Nitric Oxide
Phthalocyan..
Povidone-Iod..
Sentinox
Sodium Bicar..
pHOXWELL
SARS-CoV-2 infection typically starts in the upper respiratory
tract, and specifically the nasal respiratory epithelium. Entry via the eyes
and gastrointestinal tract is possible, but less common, and entry via other
routes is rare.
Infection may progress to the lower respiratory tract, other tissues, and the
nervous and cardiovascular systems. The primary initial route for entry into
the central nervous system is thought to be the olfactory nerve in the nasal
cavity4.
Progression may lead to cytokine storm, pneumonia, ARDS, neurological
injury5-17 and cognitive
deficits8,13, cardiovascular
complications18-22, organ failure, and death.
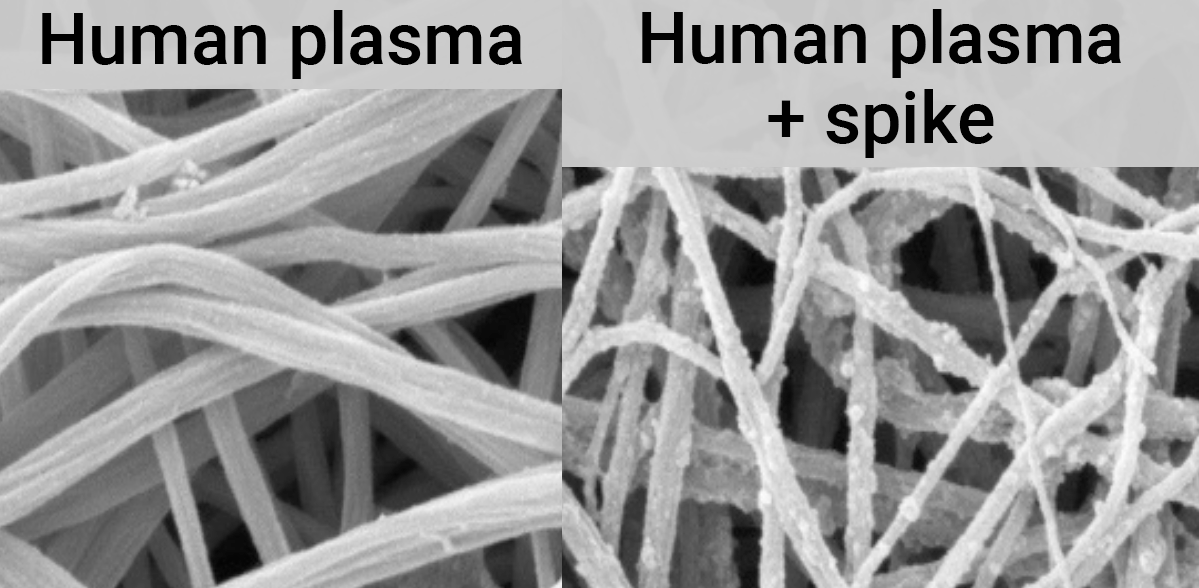
Even mild untreated infections may result in persistent cognitive
deficits23—the spike protein binds to fibrin leading to
fibrinolysis-resistant blood clots, thromboinflammation, and
neuropathology.
Systemic treatments may be insufficient to prevent
neurological damage12.
Minimizing replication as early as possible is recommended.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Logically, stopping replication in the upper respiratory tract should be
simpler and more effective.
Wu et al., using an airway organoid model incorporating many in
vivo aspects, show that SARS-CoV-2 initially attaches to cilia—hair-like
structures responsible for moving the mucus layer and where ACE2 is
localized in nasal epithelial cells26. The mucus layer and the
need for ciliary transport slow down infection, providing more time for
localized treatments24,25.
Early or prophylactic nasopharyngeal/oropharyngeal treatment may avoid the
consequences of viral replication in other tissues, and avoid the requirement
for systemic treatments with greater potential for side effects.
SARS-CoV-2 infection and replication involves the complex interplay of 100+
host and viral proteins and other factorsA,27-34, providing many
therapeutic targets for which many existing compounds have known activity.
Scientists have predicted that over 9,000 compounds may
reduce COVID-19 risk35, either by
directly minimizing infection or replication, by supporting immune system
function, or by minimizing secondary complications.
We analyze all significant
controlled studies of
iota-carrageenan
for COVID-19.
Search methods, inclusion criteria, effect extraction criteria (more serious
outcomes have priority), all individual study data, PRISMA answers, and
statistical methods are detailed in Appendix 1. We present random
effects meta-analysis results for all studies, individual outcomes, and Randomized Controlled Trials (RCTs).
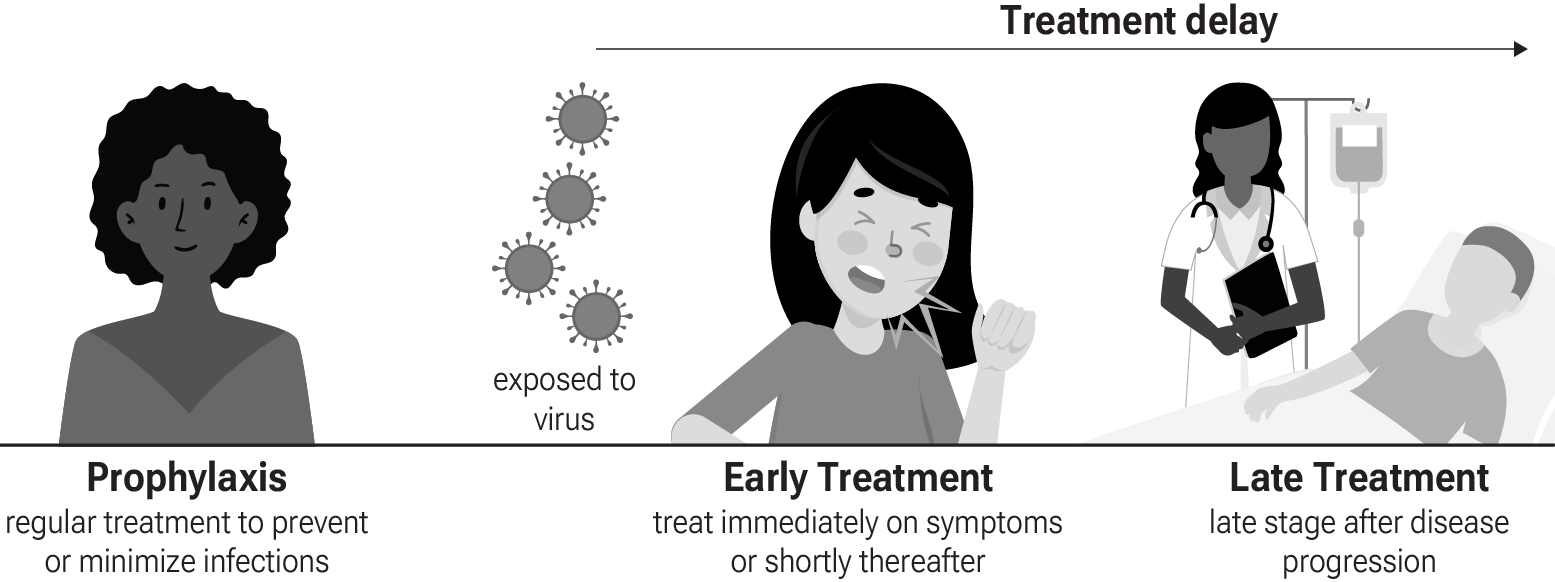
Figure 4 shows stages of possible treatment for
COVID-19. Prophylaxis refers to regularly taking medication before
becoming sick, in order to prevent or minimize infection. Early
Treatment refers to treatment immediately or soon after symptoms appear,
while Late Treatment refers to more delayed treatment.
{kind=link}
Figure 4. Treatment stages.
Preclinical research is an important part of the development of
treatments, however results may be very different in clinical trials.
Preclinical results are not used in this paper.
Table 1 summarizes the results for all studies and for Randomized Controlled Trials.
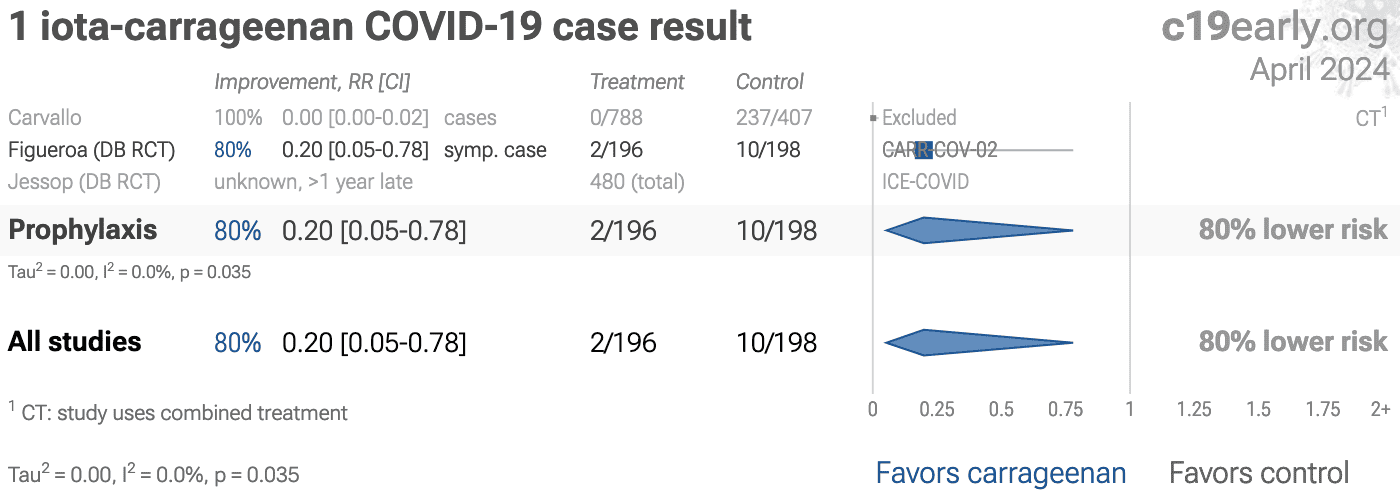
Figure 5 and 6
show forest plots for random effects meta-analysis of
all studies with pooled effects and cases.
| Relative Risk | Studies | Patients | |
|---|---|---|---|
| All studies | 0.20 [0.05‑0.78]* | 1 | 394 |
| RCTsRCTs | 0.20 [0.05‑0.78]* | 1 | 394 |
{kind=link}
{kind=link}
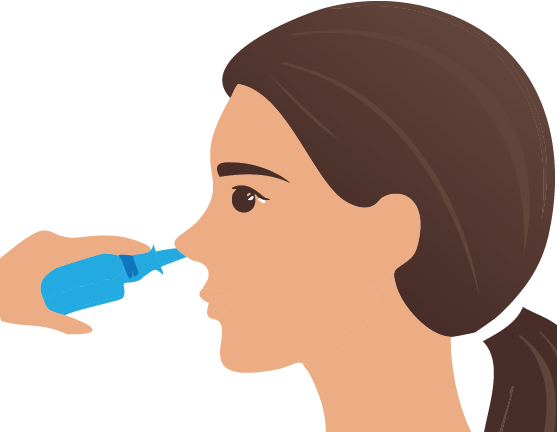
Figure 8.
Optimal spray angle may increase nasopharyngeal drug delivery 100x for nasal sprays,
adapted from Akash et al.
In addition to the dosage and frequency of administration,
efficacy for nasopharyngeal/oropharyngeal treatments may depend on many
other details. For example considering sprays, viscosity, mucoadhesion,
sprayability, and application angle are important.
Akash et al. performed a computational fluid dynamics study
of nasal spray administration showing 100x improvement in nasopharyngeal drug
delivery using a new spray placement protocol, which involves holding the spay
nozzle as horizontally as possible at the nostril, with a slight tilt towards
the cheeks. The study also found the optimal droplet size range for
nasopharyngeal deposition was ~7-17µm.
1 iota-carrageenan
RCT has not reported results1.
The trial reports
total actual enrollment of 480 patients.
The result is delayed over 2 years.
Heterogeneity in COVID-19 studies arises from many factors including:
The time between infection or the onset of symptoms and
treatment may critically affect how well a treatment works. For example an
antiviral may be very effective when used early but may not be effective in
late stage disease, and may even be harmful. Oseltamivir, for example, is
generally only considered effective for influenza when used within 0-36 or
0-48 hours52,53. Baloxavir marboxil studies for influenza
also show that treatment delay is critical — Ikematsu et al. report
an 86% reduction in cases for post-exposure prophylaxis, Hayden et al.
show a 33 hour reduction in the time to alleviation of symptoms for treatment
within 24 hours and a reduction of 13 hours for treatment within 24-48 hours,
and Kumar et al. report only 2.5 hours improvement for inpatient
treatment.
| Treatment delay | Result |
| Post-exposure prophylaxis | 86% fewer cases54 |
| <24 hours | -33 hours symptoms55 |
| 24-48 hours | -13 hours symptoms55 |
| Inpatients | -2.5 hours to improvement56 |
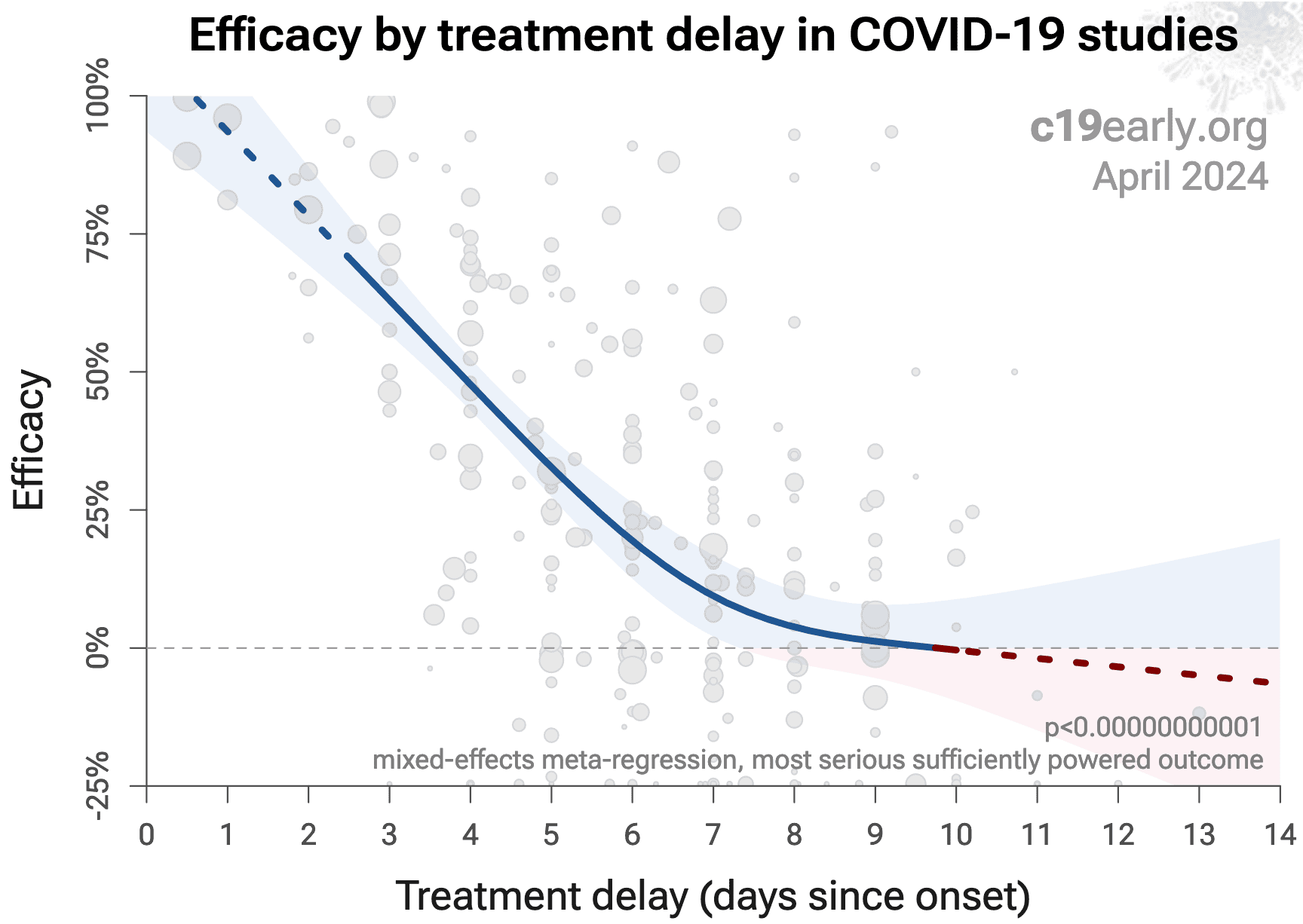
Figure 9 shows a mixed-effects meta-regression for efficacy
as a function of treatment delay in COVID-19 studies from 172 treatments, showing
that efficacy declines rapidly with treatment delay. Early treatment is
critical for COVID-19.
{kind=link}
Figure 9. Early treatment is more effective. Meta-regression showing efficacy as a function of treatment delay in COVID-19 studies from 172 treatments.
Details of the patient population including age and comorbidities may
critically affect how well a treatment works. For example, many COVID-19
studies with relatively young low-comorbidity patients show all patients
recovering quickly with or without treatment. In such cases, there is little
room for an effective treatment to improve results, for example as in
López-Medina et al.
Efficacy may depend critically on the distribution of
SARS-CoV-2 variants encountered by patients. Risk varies significantly across
variants58, for example the Gamma variant shows significantly
different characteristics59-62. Different
mechanisms of action may be more or less effective depending on variants, for
example the degree to which TMPRSS2 contributes to viral entry can differ
across variants63,64.
Effectiveness may depend strongly on the dosage and treatment regimen.
The quality of medications may vary significantly between
manufacturers and production batches, which may significantly affect efficacy
and safety. Williams et al. analyze ivermectin from 11 different sources,
showing highly variable antiparasitic efficacy across different manufacturers.
Xu et al. analyze a treatment from two different manufacturers, showing 9
different impurities, with significantly different concentrations for each
manufacturer.
Across all
studies there is a strong association between different outcomes, for example
improved recovery is strongly associated with lower mortality. However,
efficacy may differ depending on the effect measured, for example a treatment
may be more effective against secondary complications and have minimal effect
on viral clearance.
The
distribution of studies will alter the outcome of a meta analysis. Consider a
simplified example where everything is equal except for the treatment delay,
and effectiveness decreases to zero or below with increasing delay. If there
are many studies using very late treatment, the outcome may be negative, even
though early treatment is very effective.
All meta analyses combine heterogeneous studies, varying in population,
variants, and potentially all factors above, and therefore may obscure
efficacy by including studies where treatment is less effective. Generally, we
expect the estimated effect size from meta analysis to be less than that for
the optimal case.
Looking at all studies is valuable for providing an overview of all research,
important to avoid cherry-picking, and informative when a positive result is
found despite combining less-optimal situations. However, the resulting
estimate does not apply to specific cases such as
early treatment in high-risk populations.
While we present results for all studies, we also present treatment time and
individual outcome analyses, which may be more informative for specific use
cases.
Studies to date use a variety of administration methods to the
respiratory tract, including nasal and oral sprays, nasal irrigation, oral
rinses, and inhalation. Table 3 shows the relative efficacy for
nasal, oral, and combined administration. Combined administration shows the
best results, and nasal administration is more effective than oral. Precise
efficacy depends on the details of administration, e.g., mucoadhesion and
sprayability for sprays.
| Nasal/oral administration to the respiratory tract | Improvement | Studies |
| Oral spray/rinse | 38% [25‑49%] | 11 |
| Nasal spray/rinse | 58% [49‑65%] | 20 |
| Nasal & oral | 91% [74‑97%] | 7 |
Nasopharyngeal/oropharyngeal treatments may not be highly selective. In
addition to inhibiting or disabling SARS-CoV-2, they may also be harmful to
beneficial microbes, disrupting the natural microbiome in the oral cavity and
nasal passages that have important protective and metabolic roles83. This may be
especially important for prolonged use or overuse.
Table 4 summarizes the potential for common
nasopharyngeal/oropharyngeal treatments to affect the natural
microbiome.
| Treatment | Microbiome disruption potential | Notes |
|---|---|---|
| Iota-carrageenan | Low | Primarily antiviral, however extended use may mildly affect the microbiome |
| Nitric Oxide | Low to moderate | More selective towards pathogens, however excessive concentrations or prolonged use may disrupt the balance of bacteria |
| Alkalinization | Moderate | Increases pH, negatively impacting beneficial microbes that thrive in a slightly acidic environment |
| Cetylpyridinium Chloride | Moderate | Quaternary ammonium broad-spectrum antiseptic that can disrupt beneficial and harmful bacteria |
| Phthalocyanine | Moderate to high | Photodynamic compound with antimicrobial activity, likely to affect the microbiome |
| Chlorhexidine | High | Potent antiseptic with broad activity, significantly disrupts the microbiome |
| Hydrogen Peroxide | High | Strong oxidizer, harming both beneficial and harmful microbes |
| Povidone-Iodine | High | Potent broad-spectrum antiseptic harmful to beneficial microbes |
Publishing is often biased
towards positive results, however evidence suggests that there may be a negative bias for
inexpensive treatments for COVID-19. Both negative and positive results are
very important for COVID-19, media in many countries prioritizes negative
results for inexpensive treatments (inverting the typical incentive for
scientists that value media recognition), and there are many reports of
difficulty publishing positive results84-87.
For iota-carrageenan, there is currently not
enough data to evaluate publication bias with high confidence.
Pharmaceutical drug
trials often have conflicts of interest whereby sponsors or trial staff have a
financial interest in the outcome being positive. Iota-carrageenan for COVID-19
lacks this because it is off-patent, has multiple manufacturers, and is very low cost.
In contrast, most COVID-19 iota-carrageenan trials have been run by
physicians on the front lines with the primary goal of finding the best
methods to save human lives and minimize the collateral damage caused by
COVID-19. While pharmaceutical companies are careful to run trials under
optimal conditions (for example, restricting patients to those most likely to
benefit, only including patients that can be treated soon after onset when
necessary, and ensuring accurate dosing), not all iota-carrageenan trials
represent the optimal conditions for efficacy.
Summary statistics from
meta analysis necessarily lose information. As with all meta analyses, studies
are heterogeneous, with differences
in treatment delay, treatment regimen, patient demographics, variants,
conflicts of interest, standard of care, and other factors. We provide analyses for specific
outcomes and by treatment delay, and we aim to identify key characteristics in
the forest plots and summaries. Results should be viewed in the context of
study characteristics.
Some analyses classify treatment based on early or late
administration, as done here, while others distinguish between mild, moderate,
and severe cases. Viral load does not indicate degree of symptoms — for
example patients may have a high viral load while being asymptomatic. With
regard to treatments that have antiviral properties, timing of treatment is
critical — late administration may be less helpful regardless of
severity.
Details of treatment delay per patient is often not available.
For example, a study may treat 90% of patients relatively early, but the
events driving the outcome may come from 10% of patients treated very late.
Our 5 day cutoff for early treatment may be too conservative, 5 days may be too late in many cases.
Comparison across treatments is confounded by differences in
the studies performed, for example dose, variants, and conflicts of interest.
Trials with conflicts of interest may use designs better suited to the
preferred outcome.
In some cases, the most serious outcome has very few events,
resulting in lower confidence results being used in pooled analysis, however
the method is simpler and more transparent. This is less critical as the
number of studies increases. Restriction to outcomes with sufficient power may
be beneficial in pooled analysis and improve accuracy when there are few
studies, however we maintain our pre-specified method to avoid any
retrospective changes.
Studies show that combinations of treatments can be highly
synergistic and may result in many times greater efficacy than individual
treatments alone39,67-82.
Therefore standard of care may be critical and benefits may diminish or
disappear if standard of care does not include certain treatments.
This real-time analysis is constantly updated based on
submissions. Accuracy benefits from widespread review and submission of
updates and corrections from reviewers. Less popular treatments may receive
fewer reviews.
No treatment or intervention is 100% available and
effective for all current and future variants. Efficacy may vary significantly
with different variants and within different populations. All treatments have
potential side effects. Propensity to experience side effects may be predicted
in advance by qualified physicians. We do not provide medical advice. Before
taking any medication, consult a qualified physician who can compare all
options, provide personalized advice, and provide details of risks and
benefits based on individual medical history and situations.
2 of 1 studies
combine treatments. The results of
iota-carrageenan
alone may differ.
None of the RCTs use combined treatment.
Currently all studies are peer-reviewed.
SARS-CoV-2 infection and replication involves a complex
interplay of 100+ host and viral proteins and other
factors27-34, providing many therapeutic
targets.
Over 9,000 compounds have been predicted to reduce COVID-19
risk35, either by directly
minimizing infection or replication, by supporting immune system function, or
by minimizing secondary complications.
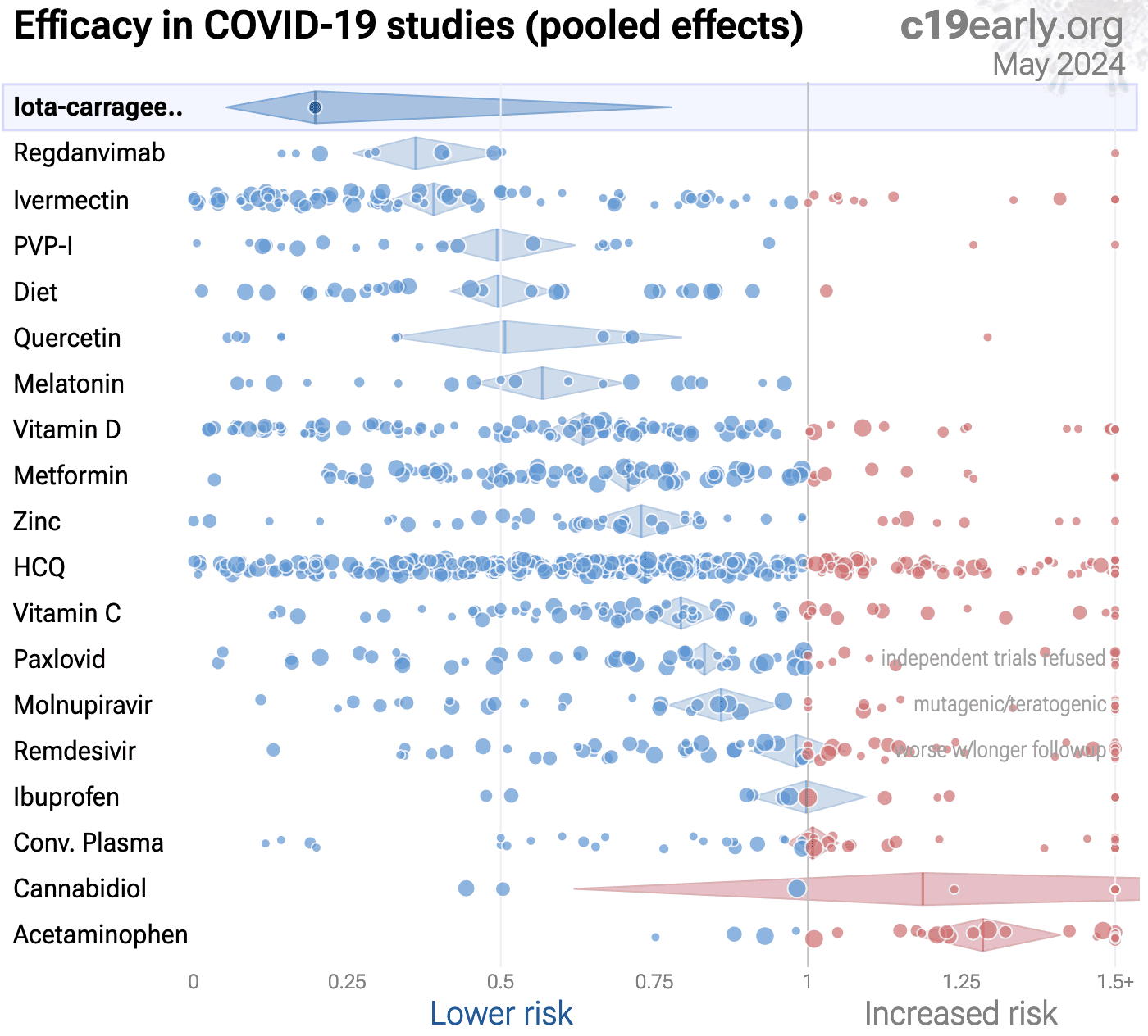
Figure 10 shows an overview of the results for iota-carrageenan
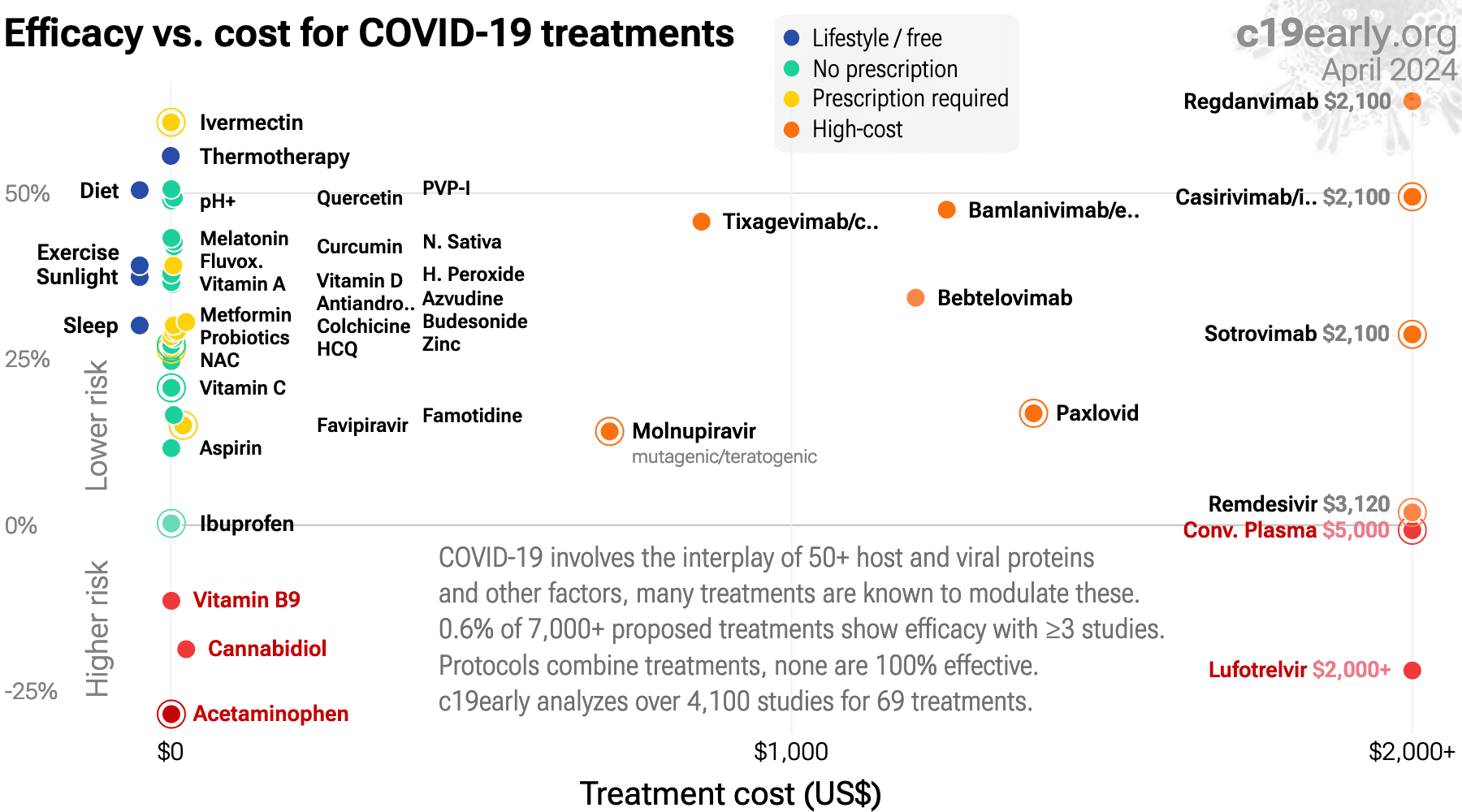
in the context of multiple COVID-19 treatments, and Figure 11 shows a plot
of efficacy vs. cost for COVID-19 treatments.
{kind=link}
Figure 10.
Scatter plot showing results within the context of multiple COVID-19 treatments.
Diamonds shows the results of random effects meta-analysis.
0.6% of 9,000+ proposed treatments show efficacy99.
{kind=link}
Figure 11. Efficacy vs. cost for COVID-19 treatments.
SARS-CoV-2 infection typically starts in the upper respiratory tract.
Progression may lead to cytokine storm, pneumonia, ARDS, neurological issues,
organ failure, and death. Stopping replication in the upper respiratory tract,
via early or prophylactic nasopharyngeal/oropharyngeal treatment, can avoid
the consequences of progression to other tissues, and avoid the requirement
for systemic treatments with greater potential for side effects.
Studies to date show that iota-carrageenan is
an effective treatment for COVID-19.
Significantly lower risk is seen for cases.
Meta analysis using the most serious outcome reported shows
80% [22‑95%] lower risk.
Currently there is very limited data, with only one study to date.
Studies have also shown efficacy with iota-carrageenan for coronavirus OC43 or 229E36, influenza A36, and rhinovirus36.
Carvallo et al. has been excluded due to combined treatments that may significantly contribute to efficacy.
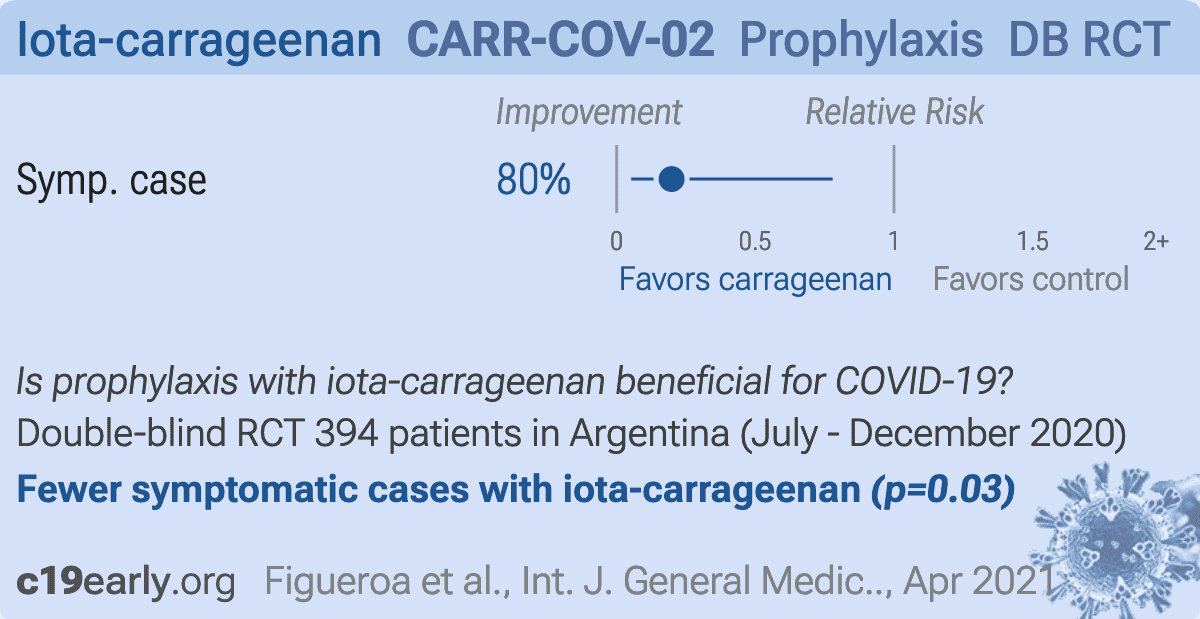{kind=link}
Prophylaxis RCT with 394 healthcare workers, 196 treated with iota-carrageenan, showing significantly lower symptomatic cases with treatment. There were no deaths or hospitalizations. There was a significant number of PCR- symptomatic cases (7.6% treatment and 8.6% control). The two treatment cases occurred shortly after randomization - infection may have occurred before the start of treatment.
480 participant iota-carrageenan prophylaxis RCT with results not reported over 2 years after completion.
We perform ongoing searches of PubMed, medRxiv, Europe PMC,
ClinicalTrials.gov, The Cochrane Library, Google Scholar, Research
Square, ScienceDirect, Oxford University Press, the reference lists of other
studies and meta-analyses, and submissions to the site c19early.org.
Search terms are iota-carrageenan and COVID-19 or SARS-CoV-2. Automated searches are performed twice daily, with all matches reviewed for inclusion.
All studies regarding the use of iota-carrageenan for COVID-19 that report
a comparison with a control group are included in the main analysis.
Studies with major unexplained data issues, for example major outcome data that
is impossible to be correct with no response from the authors, are excluded.
This is a living analysis and is updated regularly.
{kind=link}

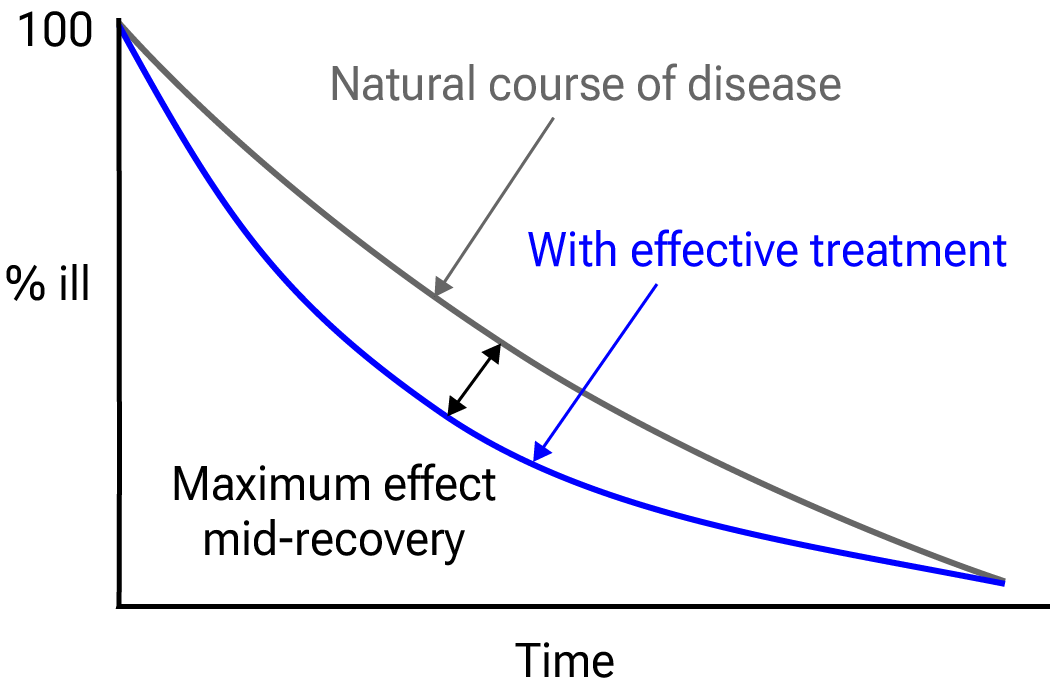
Figure 12.
Mid-recovery results can more accurately reflect efficacy when almost all patients
recover. Mateja et al. confirm that intermediate viral load results more accurately
reflect hospitalization/death.
We extracted effect sizes and associated data from all studies.
If studies report multiple kinds of effects then the most serious
outcome is used in pooled analysis, while other outcomes are included in the
outcome specific analyses. For example, if effects for mortality and cases are
reported then they are both used in specific outcome analyses, while mortality
is used for pooled analysis.
If symptomatic
results are reported at multiple times, we use the latest time, for example
if mortality results are provided at 14 days and 28 days, the results at 28
days have preference. Mortality alone is preferred over combined outcomes.
Outcomes with zero events in both arms are not used, the next most serious
outcome with one or more events is used. For example, in low-risk populations
with no mortality, a reduction in mortality with treatment is not possible,
however a reduction in hospitalization, for example, is still valuable.
Clinical outcomes are considered more important than viral outcomes.
When basically all patients recover in both treatment and control groups,
preference for viral clearance and recovery is given to results mid-recovery
where available. After most or all patients have recovered there is little or
no room for an effective treatment to do better, however faster recovery is
valuable.
An IPD meta-analysis confirms that intermediate viral load reduction
is more closely associated with hospitalization/death than later
viral load reduction100.
If only individual symptom data is available, the most serious symptom has
priority, for example difficulty breathing or low SpO2 is more
important than cough.
When results provide an odds ratio, we compute the relative risk when
possible, or convert to a relative risk according to Zhang et al.
Reported confidence intervals and p-values are used when available,
and adjusted values are used when provided. If multiple types of adjustments are
reported propensity score matching and multivariable regression has preference
over propensity score matching or weighting, which has preference over
multivariable regression. Adjusted results have preference over unadjusted
results for a more serious outcome when the adjustments significantly alter
results. When needed, conversion between reported p-values and
confidence intervals followed Altman, Altman (B), and Fisher's exact
test was used to calculate p-values for event data. If continuity
correction for zero values is required, we use the reciprocal of the opposite
arm with the sum of the correction factors equal to 1104.
Results are expressed with RR < 1.0 favoring treatment, and using the risk of
a negative outcome when applicable (for example, the risk of death rather than
the risk of survival). If studies only report relative continuous values such
as relative times, the ratio of the time for the treatment group versus the
time for the control group is used. Calculations are done in Python
(3.13.5) with
scipy (1.16.0), pythonmeta (1.26), numpy (2.3.1), statsmodels (0.14.4), and plotly (6.2.0).
Forest plots are computed using PythonMeta105
with the DerSimonian and Laird random effects model (the fixed effect
assumption is not plausible in this case) and inverse variance weighting.
Results are presented with 95% confidence intervals. Heterogeneity among studies was
assessed using the I2 statistic.
Mixed-effects meta-regression results are computed with R (4.4.0) using the metafor
(4.6-0) and rms (6.8-0) packages, and using the most serious sufficiently powered outcome.
For all statistical tests, a p-value less than 0.05 was considered statistically significant.
Grobid 0.8.2 is used to parse PDF documents.
We have classified studies as early treatment if most patients
are not already at a severe stage at the time of treatment (for example based
on oxygen status or lung involvement), and treatment started within 5 days of
the onset of symptoms. If studies contain a mix of early treatment and late
treatment patients, we consider the treatment time of patients contributing
most to the events (for example, consider a study where most patients are
treated early but late treatment patients are included, and all mortality
events were observed with late treatment patients).
We note that a shorter time may be preferable. Antivirals are typically only
considered effective when used within a shorter timeframe, for example 0-36 or
0-48 hours for oseltamivir, with longer delays not being effective52,53.
We received no funding, this research is done in our spare
time. We have no affiliations with any pharmaceutical companies or political
parties.
A summary of study results is below. Please submit
updates and corrections at https://c19early.org/gmeta.html.
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes.
For pooled analyses, the first (most serious) outcome is used, which may
differ from the effect a paper focuses on.
Other outcomes are used in outcome specific analyses.
| Carvallo (B), 11/17/2020, prospective, Argentina, peer-reviewed, 4 authors, this trial uses multiple treatments in the treatment arm (combined with ivermectin) - results of individual treatments may vary, excluded: combined treatment may significantly contribute to efficacy, concern about potential data issues. | risk of case, 99.9% lower, RR 0.001, p < 0.001, treatment 0 of 788 (0.0%), control 237 of 407 (58.2%), NNT 1.7, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| Carvallo (C), 10/19/2020, prospective, Argentina, preprint, 1 author, this trial uses multiple treatments in the treatment arm (combined with iota-carrageenan) - results of individual treatments may vary, trial NCT04425850 (history), excluded: combined treatment may significantly contribute to efficacy, concern about potential data issues. | risk of case, 96.3% lower, RR 0.04, p < 0.001, treatment 0 of 131 (0.0%), control 11 of 98 (11.2%), NNT 8.9, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| Figueroa, 4/15/2021, Double Blind Randomized Controlled Trial, Argentina, peer-reviewed, 18 authors, study period 24 July, 2020 - 20 December, 2020, trial NCT04521322 (history) (CARR-COV-02). | risk of symptomatic case, 80.2% lower, RR 0.20, p = 0.03, treatment 2 of 196 (1.0%), control 10 of 198 (5.1%), NNT 25, odds ratio converted to relative risk. | Jessop, 11/18/2022, Double Blind Randomized Controlled Trial, placebo-controlled, United Kingdom, trial NCT04590365 (history) (ICE-COVID). | 480 patient RCT with results unknown and over 2 years late. |
Viral infection and replication involves attachment, entry, uncoating and release, genome replication and transcription, translation and protein processing, assembly and budding, and release. Each step can be disrupted by therapeutics.
Jessop et al., Efficacy of Carrageenan Nasal and Throat Spray for COVID-19 Prophylaxis - A Double Blind Randomised Placebo-controlled Trial, NCT04590365, clinicaltrials.gov/study/NCT04590365.
Carvallo et al., Safety and Efficacy of the Combined Use of Ivermectin, Dexamethasone, Enoxaparin and Aspirina against COVID-19 the I.D.E.A. Protocol, Journal of Clinical Trials, 11:459 (preprint 9/15/20), www.longdom.org/open-access/safety-and-efficacy-of-the-combined-use-of-ivermectin-dexamethasone-enoxaparin-and-aspirina-against-covid19-the-idea-protocol-70290.html.
Ryu et al., Fibrin drives thromboinflammation and neuropathology in COVID-19, Nature, doi:10.1038/s41586-024-07873-4.
Dai et al., Neurological complications of COVID-19, QJM: An International Journal of Medicine, doi:10.1093/qjmed/hcac272.
Rong et al., Persistence of spike protein at the skull-meninges-brain axis may contribute to the neurological sequelae of COVID-19, Cell Host & Microbe, doi:10.1016/j.chom.2024.11.007.
Yang et al., SARS-CoV-2 infection causes dopaminergic neuron senescence, Cell Stem Cell, doi:10.1016/j.stem.2023.12.012.
Scardua-Silva et al., Microstructural brain abnormalities, fatigue, and cognitive dysfunction after mild COVID-19, Scientific Reports, doi:10.1038/s41598-024-52005-7.
Hampshire et al., Cognition and Memory after Covid-19 in a Large Community Sample, New England Journal of Medicine, doi:10.1056/NEJMoa2311330.
Duloquin et al., Is COVID-19 Infection a Multiorganic Disease? Focus on Extrapulmonary Involvement of SARS-CoV-2, Journal of Clinical Medicine, doi:10.3390/jcm13051397.
Sodagar et al., Pathological Features and Neuroinflammatory Mechanisms of SARS-CoV-2 in the Brain and Potential Therapeutic Approaches, Biomolecules, doi:10.3390/biom12070971.
Sagar et al., COVID-19-associated cerebral microbleeds in the general population, Brain Communications, doi:10.1093/braincomms/fcae127.
Verma et al., Persistent Neurological Deficits in Mouse PASC Reveal Antiviral Drug Limitations, bioRxiv, doi:10.1101/2024.06.02.596989.
Panagea et al., Neurocognitive Impairment in Long COVID: A Systematic Review, Archives of Clinical Neuropsychology, doi:10.1093/arclin/acae042.
Ariza et al., COVID-19: Unveiling the Neuropsychiatric Maze—From Acute to Long-Term Manifestations, Biomedicines, doi:10.3390/biomedicines12061147.
Vashisht et al., Neurological Complications of COVID-19: Unraveling the Pathophysiological Underpinnings and Therapeutic Implications, Viruses, doi:10.3390/v16081183.
Ahmad et al., Neurological Complications and Outcomes in Critically Ill Patients With COVID-19: Results From International Neurological Study Group From the COVID-19 Critical Care Consortium, The Neurohospitalist, doi:10.1177/19418744241292487.
Wang et al., SARS-CoV-2 membrane protein induces neurodegeneration via affecting Golgi-mitochondria interaction, Translational Neurodegeneration, doi:10.1186/s40035-024-00458-1.
Eberhardt et al., SARS-CoV-2 infection triggers pro-atherogenic inflammatory responses in human coronary vessels, Nature Cardiovascular Research, doi:10.1038/s44161-023-00336-5.
Van Tin et al., Spike Protein of SARS-CoV-2 Activates Cardiac Fibrogenesis through NLRP3 Inflammasomes and NF-κB Signaling, Cells, doi:10.3390/cells13161331.
Borka Balas et al., COVID-19 and Cardiac Implications—Still a Mystery in Clinical Practice, Reviews in Cardiovascular Medicine, doi:10.31083/j.rcm2405125.
AlTaweel et al., An In-Depth Insight into Clinical, Cellular and Molecular Factors in COVID19-Associated Cardiovascular Ailments for Identifying Novel Disease Biomarkers, Drug Targets and Clinical Management Strategies, Archives of Microbiology & Immunology, doi:10.26502/ami.936500177.
Saha et al., COVID-19 beyond the lungs: Unraveling its vascular impact and cardiovascular complications—mechanisms and therapeutic implications, Science Progress, doi:10.1177/00368504251322069.
Trender et al., Changes in memory and cognition during the SARS-CoV-2 human challenge study, eClinicalMedicine, doi:10.1016/j.eclinm.2024.102842.
Wu et al., SARS-CoV-2 replication in airway epithelia requires motile cilia and microvillar reprogramming, Cell, doi:10.1016/j.cell.2022.11.030.
Demarco, S., Shadowing SARS-CoV-2 Through Mucus and Cilia, DDN, viewonline.drugdiscoverynews.com/hubfs/DDN%20Milestones/Shadowing%20SARS-CoV-2%20Through%20Mucus%20and%20Cilia.pdf.
Lee et al., ACE2 localizes to the respiratory cilia and is not increased by ACE inhibitors or ARBs, Nature Communications, doi:10.1038/s41467-020-19145-6.
Dugied et al., Multimodal SARS-CoV-2 interactome sketches the virus-host spatial organization, Communications Biology, doi:10.1038/s42003-025-07933-z.
Malone et al., Structures and functions of coronavirus replication–transcription complexes and their relevance for SARS-CoV-2 drug design, Nature Reviews Molecular Cell Biology, doi:10.1038/s41580-021-00432-z.
Murigneux et al., Proteomic analysis of SARS-CoV-2 particles unveils a key role of G3BP proteins in viral assembly, Nature Communications, doi:10.1038/s41467-024-44958-0.
Lv et al., Host proviral and antiviral factors for SARS-CoV-2, Virus Genes, doi:10.1007/s11262-021-01869-2.
Lui et al., Nsp1 facilitates SARS-CoV-2 replication through calcineurin-NFAT signaling, Virology, doi:10.1128/mbio.00392-24.
Niarakis et al., Drug-target identification in COVID-19 disease mechanisms using computational systems biology approaches, Frontiers in Immunology, doi:10.3389/fimmu.2023.1282859.
Katiyar et al., SARS-CoV-2 Assembly: Gaining Infectivity and Beyond, Viruses, doi:10.3390/v16111648.
Wu (B) et al., Decoding the genome of SARS-CoV-2: a pathway to drug development through translation inhibition, RNA Biology, doi:10.1080/15476286.2024.2433830.
Hemilä et al., Carrageenan nasal spray may double the rate of recovery from coronavirus and influenza virus infections: Re-analysis of randomized trial data, Pharmacology Research and Perspectives, doi:10.1002/prp2.810.
Rohilla et al., Algae Polysaccharides (Carrageenan and Alginate)—A Treasure-Trove of Antiviral Compounds: An In Silico Approach to Identify Potential Candidates for Inhibition of S1-RBD Spike Protein of SARS-CoV-2, Stresses, doi:10.3390/stresses3030039.
Thet, H., The potential of carrageenan for the drug discovery of COVID-19 via molecular docking with angiotensin-converting enzyme 2 (ACE2) and the main protease (Mpro) of SARS-CoV-2, Journal of Bioinformatics and Genomics, doi:10.18454/jbg.2022.18.2.001.
Alsaidi et al., Griffithsin and Carrageenan Combination Results in Antiviral Synergy against SARS-CoV-1 and 2 in a Pseudoviral Model, Marine Drugs, doi:10.3390/md19080418.
Sattari et al., Repositioning Therapeutics for COVID-19: Virtual Screening of the Potent Synthetic and Natural Compounds as SARS-CoV-2 3CLpro Inhibitors, Research Square, doi:10.21203/rs.3.rs-37994/v1.
Yathindranath et al., Lipid Nanoparticle-Based Inhibitors for SARS-CoV-2 Host Cell Infection, International Journal of Nanomedicine, doi:10.2147/IJN.S448005.
Setz et al., Iota-Carrageenan Inhibits Replication of the SARS-CoV-2 Variants of Concern Omicron BA.1, BA.2 and BA.5, Nutraceuticals, doi:10.3390/nutraceuticals3030025.
Meister et al., Virucidal activity of nasal sprays against severe acute respiratory syndrome coronavirus-2, Journal of Hospital Infection, doi:10.1016/j.jhin.2021.10.019.
Bovard et al., Iota-carrageenan extracted from red algae is a potent inhibitor of SARS-CoV-2 infection in reconstituted human airway epithelia, Biochemistry and Biophysics Reports, doi:10.1016/j.bbrep.2021.101187.
Fröba et al., Iota-Carrageenan Inhibits Replication of SARS-CoV-2 and the Respective Variants of Concern Alpha, Beta, Gamma and Delta, International Journal of Molecular Sciences, doi:10.3390/ijms222413202.
Varese et al., Iota-carrageenan prevents the replication of SARS-CoV-2 on an in vitro respiratory epithelium model, bioRxiv, doi:10.1101/2021.04.27.441512.
Morokutti-Kurz et al., Iota-carrageenan neutralizes SARS-CoV-2 and inhibits viral replication in vitro, PLoS ONE, doi:10.1371/journal.pone.0237480.
Song et al., Inhibitory activities of marine sulfated polysaccharides against SARS-CoV-2, Food & Function, doi:10.1039/D0FO02017F.
Bansal et al., Iota-carrageenan and xylitol inhibit SARS-CoV-2 in Vero cell culture, PLoS ONE, doi:10.1371/journal.pone.0259943.
Morokutti-Kurz (B) et al., Amylmetacresol/2,4-dichlorobenzyl alcohol, hexylresorcinol, or carrageenan lozenges as active treatments for sore throat, International Journal of General Medicine, doi:10.2147/IJGM.S120665.
Akash et al., On a model-based approach to improve intranasal spray targeting for respiratory viral infections, Frontiers in Drug Delivery, doi:10.3389/fddev.2023.1164671.
Treanor et al., Efficacy and Safety of the Oral Neuraminidase Inhibitor Oseltamivir in Treating Acute Influenza: A Randomized Controlled Trial, JAMA, 2000, 283:8, 1016-1024, doi:10.1001/jama.283.8.1016.
McLean et al., Impact of Late Oseltamivir Treatment on Influenza Symptoms in the Outpatient Setting: Results of a Randomized Trial, Open Forum Infect. Dis. September 2015, 2:3, doi:10.1093/ofid/ofv100.
Ikematsu et al., Baloxavir Marboxil for Prophylaxis against Influenza in Household Contacts, New England Journal of Medicine, doi:10.1056/NEJMoa1915341.
Hayden et al., Baloxavir Marboxil for Uncomplicated Influenza in Adults and Adolescents, New England Journal of Medicine, doi:10.1056/NEJMoa1716197.
Kumar et al., Combining baloxavir marboxil with standard-of-care neuraminidase inhibitor in patients hospitalised with severe influenza (FLAGSTONE): a randomised, parallel-group, double-blind, placebo-controlled, superiority trial, The Lancet Infectious Diseases, doi:10.1016/S1473-3099(21)00469-2.
López-Medina et al., Effect of Ivermectin on Time to Resolution of Symptoms Among Adults With Mild COVID-19: A Randomized Clinical Trial, JAMA, doi:10.1001/jama.2021.3071.
Korves et al., SARS-CoV-2 Genetic Variants and Patient Factors Associated with Hospitalization Risk, medRxiv, doi:10.1101/2024.03.08.24303818.
Faria et al., Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil, Science, doi:10.1126/science.abh2644.
Nonaka et al., SARS-CoV-2 variant of concern P.1 (Gamma) infection in young and middle-aged patients admitted to the intensive care units of a single hospital in Salvador, Northeast Brazil, February 2021, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2021.08.003.
Karita et al., Trajectory of viral load in a prospective population-based cohort with incident SARS-CoV-2 G614 infection, medRxiv, doi:10.1101/2021.08.27.21262754.
Zavascki et al., Advanced ventilatory support and mortality in hospitalized patients with COVID-19 caused by Gamma (P.1) variant of concern compared to other lineages: cohort study at a reference center in Brazil, Research Square, doi:10.21203/rs.3.rs-910467/v1.
Willett et al., The hyper-transmissible SARS-CoV-2 Omicron variant exhibits significant antigenic change, vaccine escape and a switch in cell entry mechanism, medRxiv, doi:10.1101/2022.01.03.21268111.
Peacock et al., The SARS-CoV-2 variant, Omicron, shows rapid replication in human primary nasal epithelial cultures and efficiently uses the endosomal route of entry, bioRxiv, doi:10.1101/2021.12.31.474653.
Williams, T., Not All Ivermectin Is Created Equal: Comparing The Quality of 11 Different Ivermectin Sources, Do Your Own Research, doyourownresearch.substack.com/p/not-all-ivermectin-is-created-equal.
Xu et al., A study of impurities in the repurposed COVID-19 drug hydroxychloroquine sulfate by UHPLC-Q/TOF-MS and LC-SPE-NMR, Rapid Communications in Mass Spectrometry, doi:10.1002/rcm.9358.
Jitobaom et al., Favipiravir and Ivermectin Showed in Vitro Synergistic Antiviral Activity against SARS-CoV-2, Research Square, doi:10.21203/rs.3.rs-941811/v1.
Jitobaom (B) et al., Synergistic anti-SARS-CoV-2 activity of repurposed anti-parasitic drug combinations, BMC Pharmacology and Toxicology, doi:10.1186/s40360-022-00580-8.
Jeffreys et al., Remdesivir-ivermectin combination displays synergistic interaction with improved in vitro activity against SARS-CoV-2, International Journal of Antimicrobial Agents, doi:10.1016/j.ijantimicag.2022.106542.
Ostrov et al., Highly Specific Sigma Receptor Ligands Exhibit Anti-Viral Properties in SARS-CoV-2 Infected Cells, Pathogens, doi:10.3390/pathogens10111514.
Andreani et al., In vitro testing of combined hydroxychloroquine and azithromycin on SARS-CoV-2 shows synergistic effect, Microbial Pathogenesis, doi:10.1016/j.micpath.2020.104228.
De Forni et al., Synergistic drug combinations designed to fully suppress SARS-CoV-2 in the lung of COVID-19 patients, PLoS ONE, doi:10.1371/journal.pone.0276751.
Wan et al., Synergistic inhibition effects of andrographolide and baicalin on coronavirus mechanisms by downregulation of ACE2 protein level, Scientific Reports, doi:10.1038/s41598-024-54722-5.
Said et al., The effect of Nigella sativa and vitamin D3 supplementation on the clinical outcome in COVID-19 patients: A randomized controlled clinical trial, Frontiers in Pharmacology, doi:10.3389/fphar.2022.1011522.
Fiaschi et al., In Vitro Combinatorial Activity of Direct Acting Antivirals and Monoclonal Antibodies against the Ancestral B.1 and BQ.1.1 SARS-CoV-2 Viral Variants, Viruses, doi:10.3390/v16020168.
Xing et al., Published anti-SARS-CoV-2 in vitro hits share common mechanisms of action that synergize with antivirals, Briefings in Bioinformatics, doi:10.1093/bib/bbab249.
Chen et al., Synergistic Inhibition of SARS-CoV-2 Replication Using Disulfiram/Ebselen and Remdesivir, ACS Pharmacology & Translational Science, doi:10.1021/acsptsci.1c00022.
Hempel et al., Synergistic inhibition of SARS-CoV-2 cell entry by otamixaban and covalent protease inhibitors: pre-clinical assessment of pharmacological and molecular properties, Chemical Science, doi:10.1039/D1SC01494C.
Schultz et al., Pyrimidine inhibitors synergize with nucleoside analogues to block SARS-CoV-2, Nature, doi:10.1038/s41586-022-04482-x.
Ohashi et al., Potential anti-COVID-19 agents, cepharanthine and nelfinavir, and their usage for combination treatment, iScience, doi:10.1016/j.isci.2021.102367.
Al Krad et al., The protease inhibitor Nirmatrelvir synergizes with inhibitors of GRP78 to suppress SARS-CoV-2 replication, bioRxiv, doi:10.1101/2025.03.09.642200.
Thairu et al., A Comparison of Ivermectin and Non Ivermectin Based Regimen for COVID-19 in Abuja: Effects on Virus Clearance, Days-to-discharge and Mortality, Journal of Pharmaceutical Research International, doi:10.9734/jpri/2022/v34i44A36328.
Brookes et al., Mouthwash Effects on the Oral Microbiome: Are They Good, Bad, or Balanced?, International Dental Journal, doi:10.1016/j.identj.2023.08.010.
Boulware, D., Comments regarding paper rejection, twitter.com/boulware_dr/status/1311331372884205570.
Lefter et al., Polysaccharides and Lectins: A Natural Complementary Approach against the SARS-CoV-2 Pandemic, Microbiology Research, doi:10.3390/microbiolres15020035.
Chavda et al., Nasal sprays for treating COVID-19: a scientific note, Pharmacological Reports, doi:10.1007/s43440-023-00463-7.
Frediansyah, A., The antiviral activity of iota-, kappa-, and lambda-carrageenan against COVID-19: A critical review, Clinical Epidemiology and Global Health, doi:10.1016/j.cegh.2021.100826.
Hans et al., Antiviral activity of sulfated polysaccharides from marine algae and its application in combating COVID-19: Mini review, Bioresource Technology Reports, doi:10.1016/j.biteb.2020.100623.
Figueroa et al., Efficacy of a nasal spray containing Iota-Carrageenan in the prophylaxis of COVID-19 in hospital personnel dedicated to patients care with COVID-19 disease A pragmatic multicenter, randomized, double-blind, placebo-controlled trial (CARR-COV-02), International Journal of General Medicine, doi:10.2147/IJGM.S328486.
Carvallo (B) et al., Study of the Efficacy and Safety of Topical Ivermectin + Iota-Carrageenan in the Prophylaxis against COVID-19 in Health Personnel, Journal of Biomedical Research and Clinical Investigation, doi:10.31546/2633-8653.1007.
Carvallo (C) et al., Usefulness of Topic Ivermectin and Carrageenan to Prevent Contagion of Covid 19 (IVERCAR), NCT04425850, clinicaltrials.gov/ct2/show/results/NCT04425850.
Yadav et al., Therapeutic Applications of Fucoidans and their Potential to Act against COVID-19, Current Pharmaceutical Design, doi:10.2174/1381612829666221207093215.
Okechukwu et al., Marine-Derived Bioactive Metabolites as a Potential Therapeutic Intervention in Managing Viral Diseases: Insights from the SARS-CoV-2 In Silico and Pre-Clinical Studies, Pharmaceuticals, doi:10.3390/ph17030328.
Rodrigues Barbosa et al., Sulfated polysaccharides act as baits to interfere with the binding of the spike protein (SARS-CoV-2) to the ACE2 receptor and can be administered through food, Journal of Functional Foods, doi:10.1016/j.jff.2023.105532.
Eilts et al., The diverse role of heparan sulfate and other GAGs in SARS-CoV-2 infections and therapeutics, Carbohydrate Polymers, doi:10.1016/j.carbpol.2022.120167.
Mateja et al., The choice of viral load endpoint in early phase trials of COVID-19 treatments aiming to reduce 28-day hospitalization and/or death, The Journal of Infectious Diseases, doi:10.1093/infdis/jiaf282.
Zhang et al., What's the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes, JAMA, 80:19, 1690, doi:10.1001/jama.280.19.1690.
Altman (B) et al., How to obtain the confidence interval from a P value, BMJ, doi:10.1136/bmj.d2090.
Please send us corrections, updates, or comments.
c19early involves the extraction of 200,000+ datapoints from
thousands of papers. Community updates
help ensure high accuracy.
Treatments and other interventions are complementary.
All practical, effective, and safe
means should be used based on risk/benefit analysis.
No treatment or intervention is 100% available and effective for all current
and future variants.
We do not provide medical advice. Before taking any medication,
consult a qualified physician who can provide personalized advice and details
of risks and benefits based on your medical history and situation. IMA and WCH
provide treatment protocols.